For questions about the recent update for TAVNEOS® and what this means for you, please see our Letter to Providers
Severe Active Disease
- Severe vasculitis is defined by American College of Rheumatology/Vasculitis Foundation (ACR/VF) guidelines as having life-threatening or organ-threatening manifestations2
- Active vasculitis is defined by ACR/VF guidelines as new, persistent or worsening signs and/or symptoms attributed to GPA or MPA and not related to prior damage2
Identifying Patients
Approximately 80%-90% of patients with AAV present with renal or other organ-threatening disease activity, which can be considered severe active disease1,2
Patients in the ADVOCATE trial presented with a spectrum of clinical manifestations.3,4

Eyes/Mucous Membrane
Ears
Nose/throat
Cardiovascular
Chest
Abdominal
Renal
Nervous System
Cutaneous
General
Myalgia, arthralgia, fever, weight loss5,6
ADVOCATE: 20% eyes/mucous membranes involvement

Eyes/Mucous Membrane
Blurred/Loss of vision, uveites, proptosis, mouth/genetial ulcers and adnexal inflamation.
ADVOCATE: 20% eyes/mucous membranes involvement3

Ears
Conductive hearing loss, sensorineural hearing loss5,6
ADVOCATE: 43.6% ears/nose/throat involvement3

Nose/Throat
Nasal crusting and discharge, paranasal sinus involvement5,6
ADVOCATE: 43.6% ears/nose/throat involvement3

Cardiovascular
Loss of pulses, pericarditis, ischemic cardiac pain, cardiomyopathy, congestive cardiac failure5,6
ADVOCATE: 2.7% cardiovascular involvement3

Chest
Wheezing, lung nodules, infiltrates, massive hemoptysis, alveolar hemorrhage5,6
ADVOCATE: 43% chest involvement3

Abdominal
Peritonitis, bloody diarrhea, ischemic abdominal pain5,6
ADVOCATE: 1.5% abdominal involvement3

Renal
Hematuria, red cell casts, proteinuria5,6
ADVOCATE: 81.2% renal involvement3

Nervous System
Headache, meningitis, seizures, organic confusion, spinal-cord lesion, sensory peripheral neuropathy5,6
ADVOCATE: 20.9% nerves involvement3

Cutaneous
Infarct, purpura, ulcer, gangrene, other skin vasculitis5,6
ADVOCATE: 14.2% cutaneous involvement3

Careful monitoring may help detect obscure signs that your patients are experiencing severe active disease7-10
Successful identification and treatment of severe active GPA and MPA can be challenging and require a careful assessment of heterogenous symptoms10
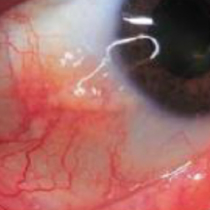
AAV with scleritis12
Image used with permission from Macarie SS, Kadar A. Rom J Ophthalmol.
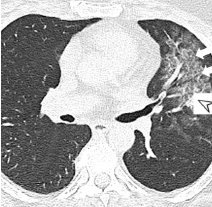
Chest computer tomography (CT) with ground-glass opacities in a patient with AAV with acute pulmonary hemorrhage13
Image used with permission from Palmucci S, Inì. C, Cosentino S, et al. Diagnostics (Basel).
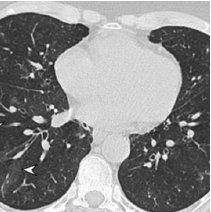
Chest CT with bilateral nodules and masses13
Image used with permission from Palmucci S, Inì. C, Cosentino S, et al. Diagnostics (Basel).

Sinonasal disease with coronal CT images showing destruction of the nasal cavity10
Image used with permission from Kitching AR, Anders H-J, Basu N, et al. Nat Rev Dis Primers.
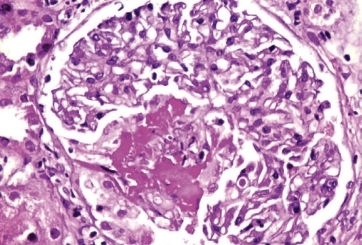
Kidney biopsy demonstrating necrotizing, pauci-immune glomerulonephritis14
Image used with permission from Vasculitis in Practice, Mohammed RHA (ed), InTechOpen, 2018.

Bilateral lower extremity purpura15
Reproduced from Purpuric lesions in a patient with ANCA-associated vasculitis, BMJ, Yang et al., 376,e065658, copyright notice 2023 with permission from BMJ Publishing Group Ltd.
AAV = ANCA-associated vasculitis; ENT = ear, nose, and throat; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis.
BVAS Overview
The Birmingham Vasculitis Activity Score (BVAS) is a clinical tool used to quantify systemic vasculitis disease activity primarily in clinical trials such as ADVOCATE16,17
There are 56 clinical features, grouped into 9 organ systems plus an “Other” category, each of which is given a numerical value according to its perceived clinical relevance as decided by expert consensus.3,16,18 Additionally, the BVAS:
- Was developed by consensus expert opinion
- Has been in use for over 25 years
- Is considered the most effective validated tool to measure systemic vasculitic disease activity
The BVAS evaluates clinical items in the following organ systems:16, 18

Renal

Nervous System

Chest

CardioVascular

Cutaneous

Mucous Membrane and eyes

Abdominal

Ear/Nose/Throat
The 9th clinical item is “general” which includes myalgia, arthralgia/arthritis, fever, weight loss.16
A higher total BVAS equates to a more active vasculitic disease at the time of evaluation.16,18
The BVAS is a validated outcome measure with demonstrated high reliability. It is efficient in terms of time and effort and is recommended for use in clinical trials.17,18
While the BVAS is primarily used in clinical trials, it may be helpful to understand the spectrum of manifestations that could indicate severe active GPA and MPA16,18
The below information is adapted from the BVAS Version 3.0. Below are the manifestations listed in the BVAS organized by organ system.6
Abdominal
- Peritonitis
- Bloody diarrhea
- Ischemic abdominal pain
Cutaneous
- Infarct
- Purpura
- Ulcer
- Gangrene
- Other skin vasculitis
Nervous System
- Headache
- Meningitis
- Organic confusion
- Seizures (not hypertensive)
- Cerebrovascular accident
- Spinal cord lesion
- Cranial nerve palsy
- Sensory peripheral neuropathy
- Mononeuritis multiplex
Cardiovascular
- Loss of pulses
- Valvular heart disease
- Pericarditis
- Ischemic cardiac pain
- Cardiomyopathy
- Congestive cardiac failure
ENT
- Bloody nasal discharge/crusts/ulcers/granulomata
- Paranasal sinus involvement
- Subglottic stenosis
- Conductive hearing loss
- Sensorineural hearing loss
Renal
- Hypertension
- Proteinuria >1+
- Hematuria ≥10 RBCs/HPF
- Serum creatinine 125-249 μmol/L*
- Serum creatinine 250-499 μmol/L*
- Serum creatinine ≥500 μmol/L*
- Rise in serum creatinine >30% or fall in creatinine clearance >25%
Chest
- Wheeze
- Nodules or cavities
- Pleural effusion/pleurisy
- Infiltrate
- Endobronchial involvement
- Massive hemoptysis/alveolar hemorrhage
- Respiratory failure
Mucous membranes/Eyes
- Mouth ulcers
- Genital ulcers
- Adnexal inflammation
- Significant proptosis
- Scleritis/Episcleritis
- Conjunctivitis/Keratitis
- Blurred vision
- Sudden visual loss
- Uveitis
- Retinal changes (vasculitis/ thrombosis/exudate/ hemorrhage)
General
- Myalgia
- Arthralgia/arthritis
- Fever ≥100.4° F
- Weight loss ≥2 kg
*Can only be scored on the first assessment.
BVAS = Birmingham Vasculitis Activity Score; GPA = granulomatosis with polyangiitis; HPF = high-power field; MPA = microscopic polyangiitis; RBC = red blood count.
Testing Considerations
Testing and diagnostic considerations in severe active GPA and MPA
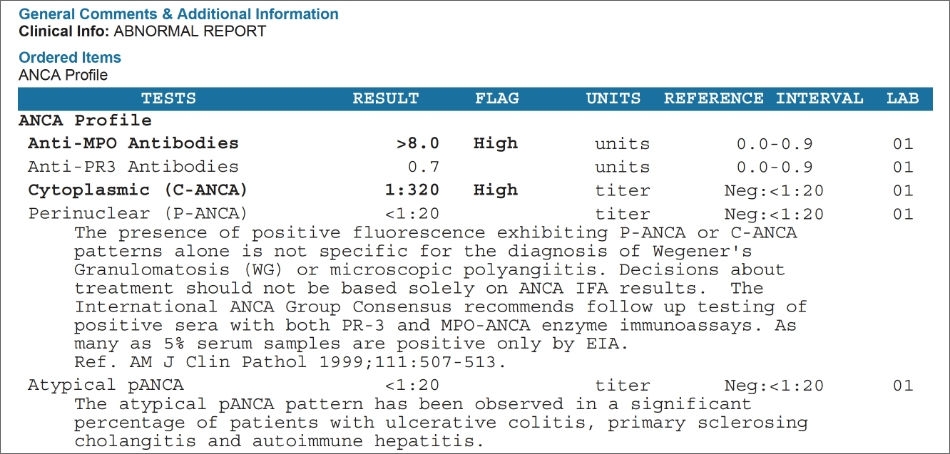
ANCA serology
- c-ANCA/PR3 antibodies are most frequently seen in GPA, and p-ANCA/MPO antibodies are most often associated with MPA7,19
- Although these antibodies are most frequently associated with respective diagnoses, ANCA positivity and specific antibodies vary by condition19
Frequency of ANCA types7
| ANCA-associated vasculitis | PR3-ANCA (mostly c-ANCA) | MPO-ANCA (mostly p-ANCA) | Other |
|---|---|---|---|
| GPA | 75% | 20% | 5% ANCA-negative |
| MPA | 30% | 60% | 10% ANCA-negative |
| ANCA-associated vasculitis | GPA |
|---|---|
| PR3-ANCA (mostly c-ANCA) | 75% |
| MPO-ANCA (mostly p-ANCA) | 20% |
| Other | 5% ANCA-negative |
| ANCA-associated vasculitis | MPA |
|---|---|
| PR3-ANCA (mostly c-ANCA) | 30% |
| MPO-ANCA (mostly p-ANCA) | 60% |
| Other | 10% ANCA-negative |
Example lab results for ANCA profile20
A full ANCA profile can be used in diagnosing
severe active GPA and MPA.
Biopsy10
Biopsy is another supportive tool that can be confirmatory, particularly in cases with renal, pulmonary, or skin involvement, but treatment should not necessarily be delayed simply to get a biopsy.
Pathology results from a kidney biopsy with AAV21
Renal biopsy in a patient with severe active AAV showing
- Severe interstitial inflammation (shown by the arrow)
- Segmental necrotizing and crescentic
glomerulonephritis (shown by the arrow)
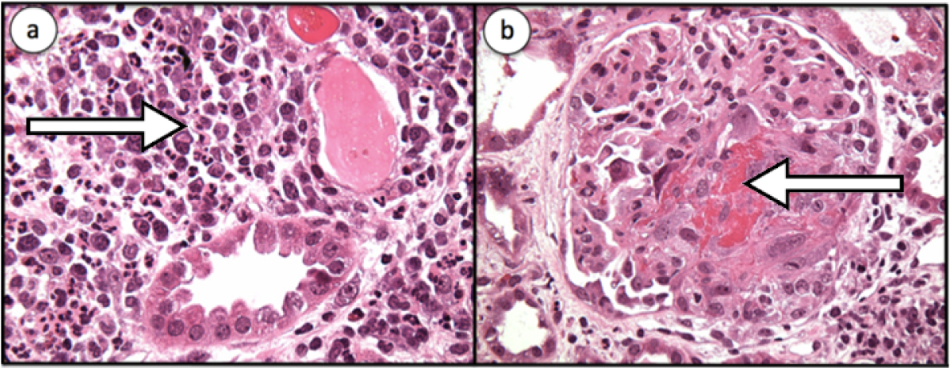
Image used with permission from Zagelbaum N, Zainab S, Gilani A, et al. Pulm Crit Care Med
AAV = ANCA-associated vasculitis; c-ANCA = cytoplasmic-ANCA; GPA = granulomatosis with polyangiitis; MPA = microscopic polyangiitis; MPO-ANCA = myeloperoxidase anti-neutrophil cytoplasmic antibody; p-ANCA = perinuclear ANCA; PR3-ANCA = proteinase (PR)3-ANCA.
ICD-10 Coding
ICD-10 codes can help identify patients with severe active GPA or MPA who may be appropriate for TAVNEOS®
This page provides a few examples of queries on electronic medical records or practice management systems that may be helpful in identifying appropriate patients for TAVNEOS®.
ICD-10 | |
|---|---|
| M31.3 | Granulomatosis with Polyangiitis (GPA)* |
| M31.30 | Granulomatosis with Polyangiitis (GPA) without renal involvement |
| M31.31 | Granulomatosis with Polyangiitis (GPA) with renal involvement |
| M31.7 | Microscopic Polyangiitis (MPA) |
| 177.6 | Unspecified Arteritis† |
| 177.82 | Anti-neutrophil cytoplasmic antibody (ANCA) vasculitis |
*GPA is formerly known as Wegener’s granulomatosis.
†The diagnosis is related to ANCA-associated vasculitis or GPA/MPA, specifically, and confirmed or awaiting confirmation using one or more lab tests: ANCA serum/biopsy/urinalysis.
ICD-10 codes and EMR can also help identify adult patients who may have undiagnosed severe active GPA or MPA
The following codes represent generalized symptoms that are common manifestations of GPA and MPA:
| ICD-10 Code | Manifestation |
|---|---|
| Vasculitic rash with systemic features | |
| L98.9 | Dermatosis |
| R23.3 | Purpuric |
| R50.9 | Fever |
| Respiratory symptoms | |
| R04.2 | Hemoptysis |
| R06.00 | Dyspnea |
| R06.02 | Shortness of breath |
| R05.9 | Cough |
| J45.909 | Asthma |
| J44.9 | Chronic |
| Renal disease | |
| N05.9 | Glomerulonephritis |
| ICD-10 Code | Manifestation |
|---|---|
| Ear, nose, throat/upper airway symptoms | |
| J32.9 | Sinusitis |
| J01.81 | Recurrent |
| H92.0 | Earache |
| H90.2 | Conductive hearing loss |
| M95.0 | Saddle nose |
| J95.5 | Subglottic stenosis |
| Eye symptoms | |
| H15.00 | Scleritis |
| H53.2 | Diplopia |
| Nerve Symptoms | |
| R20.2 | Paresthesia |
| G62.9 | Neuropathy, neuropathic |
EMR = electronic medical record; ICD-10 = International Classification of Diseases, Tenth Revision.
The information on this page is informational and is not intended to be instructive with respect to clinical decision-making or billing and coding. Healthcare providers are solely responsible for clinical decisions and ensuring the accuracy and validity of all billing and claims. This is not a guarantee of coverage or reimbursement for any product or service.